
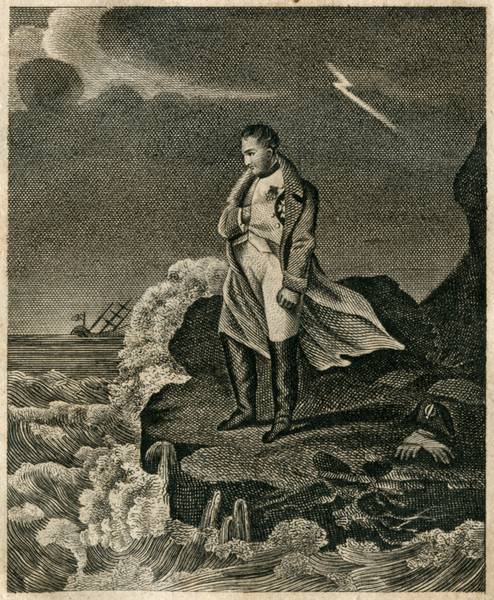
Napoleon’s Exile.

The first abdication was originally conditional. Tsar Alexander had then proposed that Napoleon be exiled to Elba. Even after the unconditional abdication, the marquis de Caulaincourt convinced Alexander to keep the proposition open. Napoleon wasn’t seen as a criminal, an upstart perhaps, but his rule was legitimate and the wars were often declared by the Coalition.
There wasn’t widespread support for Elba, and most diplomats and politicians had their own ideas on where to send him. The United States, Corsica, Sardinia, and the British fort of St. George on Beauly Firth were other possibilities. Alexander insisted on Elba as it would put him at an advantage to Austrian interests, and the other nations went along with it due to the other choices not being entirely pleasing — along with some threats from Alexander that were Napoleon not sent to Elba he would rescind his support for the Bourbons.
When Napoleon escaped, he was declared as much as an enemy of humanity and that he would banished from Europe if captured. He could, in theory, be executed. After Napoleon’s defeat at Waterloo, the Prussians stated that he would be executed if captured by them. For personal reasons, Napoleon refused to surrender to the Austrians and Russians — though they were unlikely to execute him. Napoleon made his way to Rochefort where he planned on embarking to the United States, though he delayed in doing so and the British blockaded the port in the meantime. Napoleon sent his aides to the captain of the HMS Bellerophon to see what terms he might get for surrendering to them. Captain Maitland suggested that asylum in England may be possible, but would have to clear it.
After some deliberation, Napoleon decided to surrender himself to the Bellerophon. When it arrived at Torbay, Napoleon was kept on board — an amusement for sight seers to come and see. The British government debated what to do with him. The three main figures (being the Prince Regent, Prime Minister, and Secretary of War) all hated him and previously instructed the Bourbons that they should execute him. They declared Napoleon a prisoner of war, which put Bonaparte in a grey area of legality. He couldn’t technically be a prisoner of war since Britain and France were no longer at war. Napoleon was no longer considered to even be a citizen of France. The possibility of him being tried and executed as an outlaw or pirate was raised, but then he couldn’t have been detained as a prisoner of war.
The government’s response to this scenario was to exile Napoleon to St. Helena as a retired general on half pay. Napoleon’s response to this was bewilderment and confusion, stating that if his coming aboard the Bellerophon was simply a trick to make him a prisoner, Britain had shamed itself. One of his remarks was, “They may as well call me Archbishop, for I was head of the Church as well as the army.” The Allies approved of the action, though the British Parliament later admitted that the government had no legal basis for Napoleon’s exile.
So, specifically as for why Napoleon wasn’t executed basically comes down to the unique position he was in. The concept of war criminals wasn’t yet around, and Napoleon was neither a figure that could simply be executed nor given asylum. If Napoleon had been given a *writ of habeus corpus, he could have been put on trial. However, the British government didn’t want the possibility for Napoleon to be let off, so they quickly decided to exile him. Even that was outside of their legal jurisdiction, but it caused a lot less fallout than an execution would have.
[*Napoleon technically had received a writ of habeus corpus. A sympathetic former judge came up with an excuse (an admiral failing to perform his duties) to have Napoleon appear as a witness in a trial. The writ was obtained, but Napoleon was whisked away before he could set foot on land.]
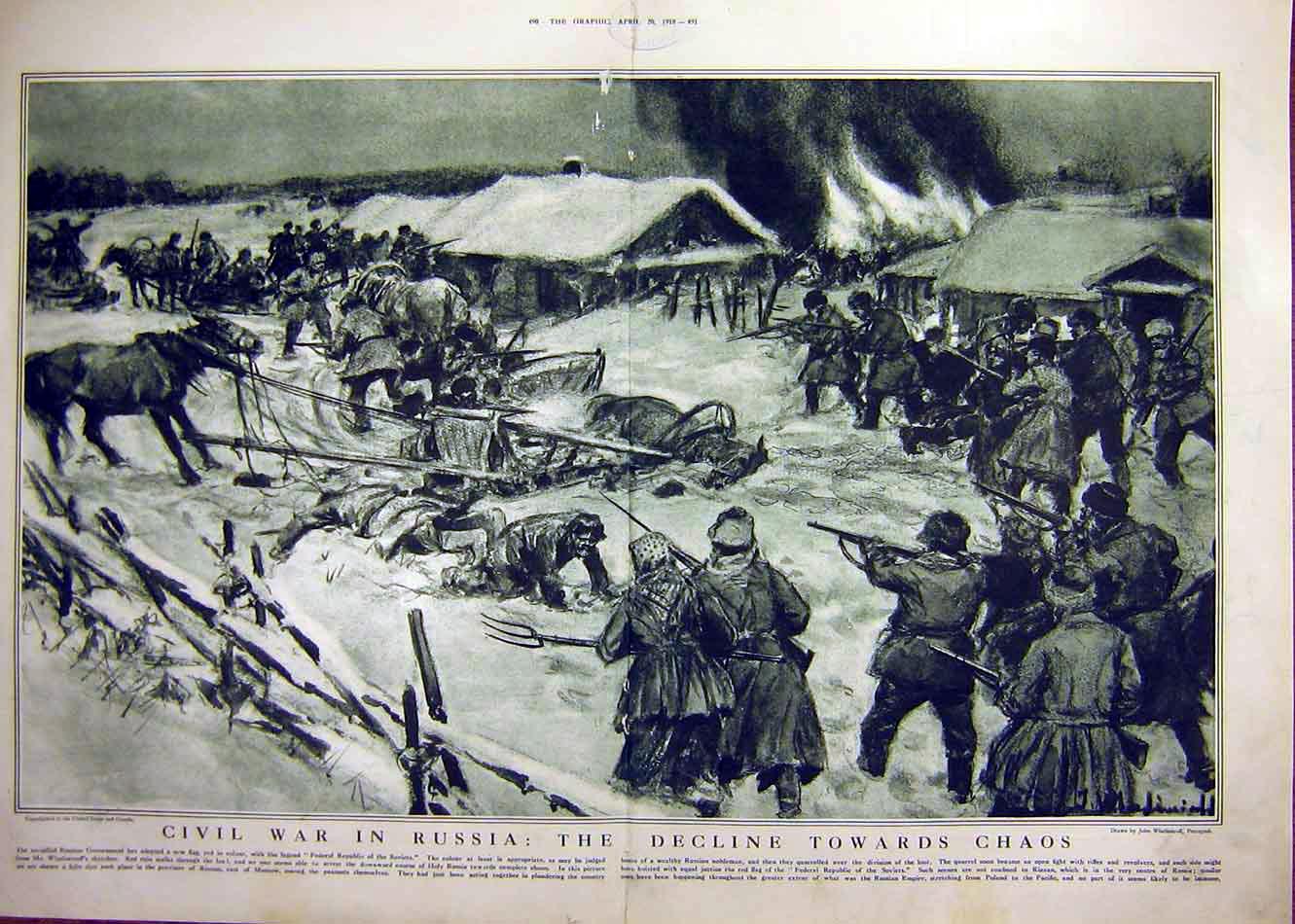
American intervention in the Russian Civil War:
 American involvement in Russia was part of an Allied Intervention into Russia rather than an actual invasion. President Wilson authorized limited military force in Russia but no formal declaration of war was ever authorized by the American Congress. Wilson ordered 5,000 men to occupy Arkhangelsk and around 8,000 to Vladivostok, a port city on the far eastern reaches of Russia. The American “expeditionary” forces were not part of a concerted American war effort but rather an American commitment made out of the emerging European debates that followed the First World War. Wilson was also known to use limited occupational forces to achieve political goals. One example is his 1914 occupation of the Mexican port city Veracruz to influence the success of a U.S. friendly Mexican government, obviously Veracruz is a different story but it demonstrates that Wilson used Executive power to authorize military occupations that were not necessarily outright invasions or declarations of war.
American involvement in Russia was part of an Allied Intervention into Russia rather than an actual invasion. President Wilson authorized limited military force in Russia but no formal declaration of war was ever authorized by the American Congress. Wilson ordered 5,000 men to occupy Arkhangelsk and around 8,000 to Vladivostok, a port city on the far eastern reaches of Russia. The American “expeditionary” forces were not part of a concerted American war effort but rather an American commitment made out of the emerging European debates that followed the First World War. Wilson was also known to use limited occupational forces to achieve political goals. One example is his 1914 occupation of the Mexican port city Veracruz to influence the success of a U.S. friendly Mexican government, obviously Veracruz is a different story but it demonstrates that Wilson used Executive power to authorize military occupations that were not necessarily outright invasions or declarations of war.
Importantly the number of around 13,000 thousand American soldiers was considerably less than the commitments of Czechoslovakia’s (50,000), France’s (12,000) and Britain’s (40,000). Moreover the strategic importance of the areas occupied by America were also minor in comparison to other zones of conflict and the role of America was manifestly less significant than the contributions of her Allies. General Graves who commanded the American contingent present in Siberia (American Expeditionary Force Siberia) had the aim of protecting American military equipment and American capital investment that was still in Russia after the abdication of Tsar Nicholas II. Graves’ other objectives included safe guarding the exit of the Czech legion from Russian territory and to assist the reorganization of the new Russian government.
You have to take into account that Russia in 1918 was vastly different from the Communist state that we understand it to have been throughout the twentieth century. In 1918 it was not clear that the Bolsheviks would emerge as victors, the Red Army faced opponents on four fronts to control a comparatively small area compared to the huge country we know Russia is today. The map I’ve linked at the bottom shows the extent of Bolshevik control in 1919, Archangelsk is just at the top, Vladivostok where most of the Americans were stationed is located thousands of kilometers to the east and Americans stationed there engaged in a limited role against Russian Cossacks, a group separate to the Revolutionary Bolsheviks.
Wilson’s motivations for sending American troops were numerous but stemmed from his willingness to see through his own vision for a post war peace process. He was pressured by allies to commit to Russian intervention and he likely did so in a diplomatic measure to ensure he had some leverage in the Paris Peace Conference in 1919. Undoubtedly Wilson was more concerned with fostering a democratic environment in Europe (and protecting physical American interests in Russia) rather than in participating in a huge mobilization against Russia after the toll of the First World War. The intervention was certainly no secret, Congressmen, Newspapers and Citizens were alert to the experiences of American soldiers stationed in the frozen port cities and campaigned for the men to be returned. Generally Americans opposed intervention and largely felt that their commitment in the First World War had been sufficient enough in aiding allied European nations. Additionally many Americans did not share the international spirit that Wilson pushed in the post-war peace conferences. President Warren Harding who followed Wilson’s administration condemned the intervention as a complete mistake.
Here are a couple of good sources if you want to develop some of the ideas that I’ve written here:
(It wasn’t an invasion, it was an intervention authorized by the President and not Congress and the American people knew about it.)

*Maybe the best quick read to get the bet settled that isn’t a wikipedia article.
*The introduction here will help you get a better idea on some of the context surrounding the intervention.

Hobby Lobby SCOTUS Ruling:
The Supreme Court ruling on BURWELL, SECRETARY OF HEALTH AND HUMAN SERVICES, ET AL. v. HOBBY LOBBY STORES, INC. has now opened up the precedent (ignoring how narrowly tailored the ruling was to only contraception) that under the RFRA, even if its a compelling government interest, the state cannot mandate any firm with sincere religious beliefs to carry out a requirement, so long as the government can pick up the slack? It seems like the least restrictive means will always be making the government do it instead and not restrict at all anyone’s religious beliefs.
On page 46 of the opinion, Alito writes: “Our decision should not be understood to hold that an insurance-coverage mandate must necessarily fall if it conflicts with an employer’s religious beliefs. Other coverage requirements, such as immunizations, may be supported by different interests (for example, the need to combat the spread of infectious diseases) and may involve different arguments about the least restrictive means of providing them.”
This certainly leaves open the possibility that the Court could rule differently on the “least restrictive means” issue in the future, but his language in section V-B, which discusses the “least restrictive means” test, seems to indicate that it is a difficult standard to pass. On page 41 of the opinion, he indicates that “the most straightforward way of [meeting the least restrictive means test] would be for the Government to assume the cost.” He also says that “HHS has not shown … that this is not a viable alternative.” This seems to indicate that if such a challenge were to come up regarding vaccination or blood transfusions, or whatever else, the burden would be on the Department of Health and Human Services to show that it would be impractical for the Government to cover the cost. That would be quite the burden for the Government to prove.
Ginsberg seems to agree with that reading in her dissent. On page 29 on the dissent, she writes, “And where is the stopping point to the ‘let the government pay’ alternative? Suppose an employer’s sincerely held religious belief is offended by health coverage of vaccines, or paying the minimum wage, … or according women equal pay for substantially similar work…? Does it rank as a less restrictive alternative to require the government to provide the money or benefit to which the employer has a religion-based objection?” In addition to indicating that the Court’s logic could prove problematic in the future, she asserts that it is flawed at present, saying, “In sum, in view of what Congress sought to accomplish, i.e., comprehensive preventive care for women furnished through employer-based health plans, none of the proffered alternatives would satisfactorily serve the compelling interests to which Congress responded.”
I agree with Justice Ginsberg on many points here, especially the last few pages of her dissent. Justice Alito attempts to narrow his ruling as much as possible, but leaves a lot of questions unanswered as to the basis for his narrow ruling. To me, the most compelling arguments come from sections III-4 and IV (pages 27-35) of Ginsberg’s dissent. She basically asserts that the Court’s ruling has much broader implications than it intends, and poses quite a few questions about the basis for the narrow ruling.
I am also inclined to agree with her reasoning that the Court should have no business in determining which religious views are legitimate and which are not, and that religious exemptions from generally applicable law should be reserved for groups that are organized “for a religious purpose” and/or “engaged primarily in carrying out that religious purpose”.
The Supreme Court ruling can be found here: http://www.supremecourt.gov/opinions/13pdf/13-354_olp1.pdf
Justice Ginsburg’s dissent here: http://www.scribd.com/mobile/doc/231974154

History of Abortion
The following is an excerpt from the “Abortion” chapter of Our Bodies, Ourselves for the New Century.

HISTORY OF ABORTION
Over several centuries and in different cultures, there is a rich history of women helping each other to abort. Until the late 1800s, women healers in Western Europe and the U.S. provided abortions and trained other women to do so, without legal prohibitions.
The State didn’t prohibit abortion until the 19th century, nor did the Church lead in this new repression. In 1803, Britain first passed antiabortion laws, which then became stricter throughout the century. The U.S. followed as individual states began to outlaw abortion. By 1880, most abortions were illegal in the U.S., except those “necessary to save the life of the woman.” But the tradition of women’s right to early abortion was rooted in U.S. society by then; abortionists continued to practice openly with public support, and juries refused to convict them.
Abortion became a crime and a sin for several reasons. A trend of humanitarian reform in the mid-19th century broadened liberal support for criminalization, because at that time abortion was a dangerous procedure done with crude methods, few antiseptics, and high mortality rates. But this alone cannot explain the attack on abortion. For instance, other risky surgical techniques were considered necessary for people’s health and welfare and were not prohibited. “Protecting” women from the dangers of abortion was actually meant to control them and restrict them to their traditional child-bearing role. Antiabortion legislation was part of an antifeminist backlash to the growing movements for suffrage, voluntary motherhood, and other women’s rights in the 19th century. *For more information, see Linda Gordon’s Woman’s Body, Woman’s Right, rev. ed. (New York: Penguin Books, 1990).
At the same time, male doctors were tightening their control over the medical profession. Doctors considered midwives, who attended births and performed abortions as part of their regular practice, a threat to their own economic and social power. The medical establishment actively took up the antiabortion cause in the second half of the 19th century as part of its effort to eliminate midwives.
Finally, with the declining birth rate among whites in the late 1800s, the U.S. government and the eugenics movement warned against the danger of “race suicide” and urged white, native-born women to reproduce. Budding industrial capitalism relied on women to be unpaid household workers, low-paid menial workers, reproducers, and socializers of the next generation of workers. Without legal abortion, women found it more difficult to resist the limitations of these roles.
Then, as now, making abortion illegal neither eliminated the need for abortion nor prevented its practice. In the 1890s, doctors estimated that there were two million abortions a year in the U.S. (compared with one and a half million today). Women who are determined not to carry an unwanted pregnancy have always found some way to try to abort. All too often, they have resorted to dangerous, sometimes deadly methods, such as inserting knitting needles or coat hangers into the vagina and uterus, douching with dangerous solutions like lye, or swallowing strong drugs or chemicals. The coat hanger has become a symbol of the desperation of millions of women who have risked death to end a pregnancy. When these attempts harmed them, it was hard for women to obtain medical treatment; when these methods failed, women still had to find an abortionist.
Illegal Abortion
Many of us do not know what it was like to need an abortion before legalization. Women who could afford to pay skilled doctors or go to another country had the safest and easiest abortions. Most women found it difficult if not impossible to arrange and pay for abortions in medical settings.
With one exception, the doctors whom I asked for an abortion treated me with contempt, their attitudes ranging from hostile to insulting. One said to me, “You tramps like to break the rules, but when you get caught you all come crawling for help in the same way.”
The secret world of illegal abortion was mostly frightening and expensive. Although there were skilled and dedicated laywomen and doctors who performed safe, illegal abortions, most illegal abortionists, doctors, and those who claimed to be doctors cared only about being well rewarded for their trouble. In the 1960s, abortionists often turned women away if they could not pay $1,000 or more in cash. Some male abortionists insisted on having sexual relations before the abortion.
Abortionists emphasized speed and their own protection. They often didn’t use anesthesia because it took too long for women to recover, and they wanted women out of the office as quickly as possible. Some abortionists were rough and sadistic. Almost no one took adequate precautions against hemorrhage or infection.
Typically, the abortionist would forbid the woman to contact him or her again. Often she wouldn’t know his or her real name. If a complication occurred, harassment by the law was a frightening possibility. The need for secrecy isolated women having abortions and those providing them.
In the 1950s, about a million illegal abortions a year were performed in the U.S., and over a thousand women died each year as a result. Women who were victims of botched or unsanitary abortions came in desperation to hospital emergency wards, where some died of widespread abdominal infections. Many women who recovered from such infections found themselves sterile or chronically and painfully ill. The enormous emotional stress often lasted a long time.
Poor women and women of color ran the greatest risks with illegal abortions. In 1969, 75% of the women who died from abortions (most of them illegal) were women of color. Of all legal abortions in that year, 90% were performed on white private patients.
The Push for Legal Abortion
In the 1960s, inspired by the civil rights and antiwar movements, women began to fight more actively for their rights. The fast-growing women’s movement took the taboo subject of abortion to the public. Rage, pain, and fear burst out in demonstrations and speakouts as women burdened by years of secrecy got up in front of strangers to talk about their illegal abortions. Women marched and rallied and lobbied for abortion on demand. Civil liberties groups and liberal clergy joined in these efforts to support women.
Reform came gradually. A few states liberalized abortion laws, allowing women abortions in certain circumstances (e.g., pregnancy resulting from rape or incest, being under 15 years of age) but leaving the decision up to doctors and hospitals. Costs were still high and few women actually benefited.
In 1970, New York State went further, with a law that allowed abortion on demand through the 24th week from the LMP if it was done in a medical facility by a doctor. A few other states passed similar laws. Women who could afford it flocked to the few places where abortions were legal. Feminist networks offered support, loans, and referrals and fought to keep prices down. But for every woman who managed to get to New York, many others with limited financial resources or mobility did not. Illegal abortion was still common. The fight continued; several cases before the Supreme Court urged the repeal of all restrictive state laws.
On January 22, 1973, the U.S. Supreme Court, in the famous Roe v. Wadedecision, stated that the “right of privacy…founded in the Fourteenth Amendment’s concept of personal liberty…is broad enough to encompass a woman’s decision whether or not to terminate her pregnancy.” The Court held that through the end of the first trimester of pregnancy, only a pregnant woman and her doctor have the legal right to make the decision about an abortion. States can restrict second-trimester abortions only in the interest of the woman’s safety. Protection of a “viable fetus” (able to survive outside the womb) is allowed only during the third trimester. If a pregnant woman’s life or health is endangered, she cannot be forced to continue the pregnancy.
Abortion After Legalization
Though Roe v. Wade left a lot of power to doctors and to government, it was an important victory for women. Although the decision did not guarantee that women would be able to get abortions when they wanted to, legalization and the growing consciousness of women’s needs brought better, safer abortion services. For the women who had access to legal abortions, severe infections, fever, and hemorrhaging from illegal or self- induced abortions became a thing of the past. Women health care workers improved their abortion techniques. Some commercial clinics hired feminist abortion activists to do counseling. Local women’s groups set up public referral services, and women in some areas organized women-controlled nonprofit abortion facilities. These efforts turned out to be just the beginning of a longer struggle to preserve legal abortion and to make it accessible to all women.
Although legalization greatly lowered the cost of abortion, it still left millions of women in the U.S., especially women of color and young, rural women, and/or women with low incomes, without access to safe, affordable abortions. State regulations and funding have varied widely, and second-trimester abortions are costly. Even when federal Medicaid funds paid for abortions, fewer than 20% of all public county and city hospitals actually provided them. This meant that about 40% of U.S. women never benefited from liberalized abortion laws.
During the late 1970s and early 1980s, feminist health centers around the country provided low-cost abortions that emphasized quality of care, and they maintained political involvement in the reproductive rights movement. Competition from other abortion providers, harassment by the IRS, and a profit- oriented economy made their survival difficult. By the early 1990s, only 20 to 30 of these centers remained.
Eroding Abortion Rights: After Roe v. Wade
When the Supreme Court legalized abortion in 1973, the antiabortion forces, led initially by the Catholic Church hierarchy, began a serious mobilization using a variety of political tactics including pastoral plans, political lobbying, campaigning, public relations, papal encyclicals, and picketing abortion clinics. The Church hierarchy does not truly represent the views of U.S. Catholics on this issue or the practice of Catholic women, who have abortions at a rate slightly higher than the national average for all women.
Other religious groups, like the Mormons and some representatives of Jewish orthodoxy, have traditionally opposed abortion. In the 1980s, rapidly growing fundamentalist Christian groups, which overlap with the New Right and “right- to-life” organizations, were among the most visible boosters of the antiabortion movement. These antiabortion groups talk as if all truly religious and moral people disapprove of abortion. This is not true now and never has been.
The long-range goal of the antiabortion movement is to outlaw abortion. Their short-range strategy has been to attack access to abortion, and they have had successes. The most vulnerable women–young women; women with low incomes, of whom a disproportionate number are women of color; all women who depend on the government for their health care–have borne the brunt of these attacks on abortion rights.
The antiabortion movement’s first victory, a major setback to abortion rights, came in July 1976, when Congress passed the Hyde Amendment banning Medicaid funding for abortion unless a woman’s life was in danger. Following the federal government, many states stopped funding “medically unnecessary” abortions. The result was immediate in terms of harm and discrimination against women living in poverty. In October 1977, Rosie Jimeaanez, a Texas woman, died from an illegal abortion in Mexico, after Texas stopped funding Medicaid abortions.
It is impossible to count the number of women who have been harmed by the Hyde Amendment, but before Hyde, one-third of all abortions were Medicaid funded: 294,000 women per year. (Another 133,000 Medicaid-eligible women who needed abortions were unable to gain access to public funding for the procedure.) Without state funding, many women with unwanted pregnancies are forced to have babies, be sterilized, or have abortions using money needed for food, rent, clothing, and other necessities.
Although a broad spectrum of groups fought against the Hyde Amendment, countering this attack on women who lack financial resources was not a priority of the pro-choice movement. There was no mass mobilization or public outcry. In the long run, this hurt the pro-choice movement, as the attack on Medicaid funding was the first victory in the antiabortion movement’s campaign to deny access to abortion for all women.
Young women’s rights have been a particular target of the antiabortion movement. About 40% of the one million teens who become pregnant annually choose abortion. Parental involvement laws, requiring that minors seeking abortions either notify their parents or receive parental consent, affect millions of young women. As of early 1997, 35 states have these laws; 23 states enforce them. In some states, a physician is required to notify at least one parent either in person, by phone, or in writing. Health care providers face loss of license and sometimes criminal penalties for failure to comply.
Antiabortion forces have also used illegal and increasingly violent tactics, including harassment, terrorism, violence, and murder. Since the early 1980s, clinics and providers have been targets of violence. Over 80% of all abortion providers have been picketed or seriously harassed. Doctors and other workers have been the object of death threats, and clinics have been subject to chemical attacks (for example, butyric acid), arson, bomb threats, invasions, and blockades. In the late 1980s, a group called Operation Rescue initiated a strategy of civil disobedience by blockading clinic entrances and getting arrested. There were thousands of arrests nationwide as clinics increasingly became political battlefields.
In the 1990s, antiabortionists increasingly turned to harassment of individual doctors and their families, picketing their homes, following them, and circulating “Wanted” posters. Over 200 clinics have been bombed. After 1992, the violence became deadly. The murder of two doctors and an escort at a clinic in Pensacola, Florida, was followed by the murder of two women receptionists at clinics in Brookline, Massachusetts. A health care provider spoke about the impact of the violence:
The fear of violence has become part of the lives of every abortion provider in the country. As doctors, we are being warned not to open big envelopes with no return addresses in case a mail bomb is enclosed. I know colleagues who have had their homes picketed and their children threatened. Some wear bullet-proof vests and have remote starters for their cars. Even going to work and facing the disapproving looks from co-workers–isolation and marginalization from colleagues is part of it.
The antiabortion movement continues to mount new campaigns on many fronts. Most recently, it has aggressively put out the idea that abortion increases the risk of breast cancer. In January 1997, the results of a Danish study, the largest to date (involving one and a half million women), showed that there is no connection.s3 Unlike previous studies, this one did not rely on interviews and women’s reports but instead used data obtained from population registries about both abortion and breast cancer. Despite the lack of medical evidence and the fact that the scientific community does not recognize any link, the antiabortion movement continues to stir up fears about abortion and breast cancer.
Legal but Out of Reach for Many Women
We have learned that legalization is not enough to ensure that abortions will be available to all women who want and need them. In addition to a lack of facilities and trained providers, burdensome legal restrictions, including parental consent or notification laws for minors and mandatory waiting periods, create significant obstacles. A minor who has been refused consent by a parent may have to go through an intimidating and time-consuming judicial hearing. Mandatory waiting periods may require a woman to miss extra days of work because she must go to the clinic not once, but twice, to obtain an abortion. If travel is required, this can make the whole procedure unaffordable. In other words, for millions of women, youth, race, and economic circumstances together with the lack of accessible services–especially for later abortions–translate into daunting barriers, forcing some women to resort to unsafe and illegal abortions and self-abortions.
WEAKENING THE CONSTITUTIONAL PROTECTION FOR ABORTION
When in 1980 the Supreme Court upheld the Hyde Amendment, it began eroding the constitutional protection for abortion rights. Since then, there have been other severe blows. In Webster v. Reproductive Health Services (1989), the Court opened the door to new state restrictions on abortion. In Hodgson v. Minnesota (1990), the Court upheld one of the strictest parental notification laws in the country.
These trends were further codified in Planned Parenthood v. Casey, a 1992 decision upholding a highly restrictive Pennsylvania law that included mandatory waiting periods and mandatory biased counseling. Two frightening themes emerged in the Casey decision. First, the Court sanctioned the view that government may regulate the health care of pregnant women to protect fetal life from the moment of conception so long as it does not “unduly burden” access to an abortion. Second, the Court showed little concern for the severe impact of state restrictions on women with few financial resources.
In the aftermath of Casey, many states have passed similar restrictions, which have the effect of limiting access to abortion, especially for women with low incomes, teenage women, and women of color.
These infringements on abortion access have curtailed the abortion rights of millions of women. In the face of the unrelenting efforts of the antiabortion movement, those of us who believe that women should make their own reproductive decisions will have to become involved in the ongoing struggle to preserve and expand abortion rights.
REPRODUCTIVE FREEDOM VS. POPULATION CONTROL
While most women’s health groups see the fight for abortion rights in the context of defending the rights of all women to make their own decisions about reproduction, not all advocates of abortion rights share this understanding. Some view legal abortion and contraception as tools of population control.
Advocates of population control blame overpopulation for a range of problems, from global poverty to ethnic conflict and environmental degradation. Historically, this type of thinking has led to a range of coercive fertility control policies that target Third World women. These include sterilization without a woman’s knowledge or consent; the use of economic incentives to “encourage” sterilization, a practice that undermines the very notion of reproductive choice; the distribution and sometimes coercive or unsafe use of contraceptive methods, often without appropriate information; the denial of abortion services; and sometimes coercive abortion. For example, HIV-positive women in the U.S. (who are overwhelmingly women of color) are often pressured to have abortions, though only 20 to 25% of their children will be HIV-positive and new treatments during pregnancy have reduced the likelihood even further.
Women with few economic resources, especially women of color in the U.S. and throughout the world, have been the primary targets of population control policies. For example, although abortion has become increasingly less accessible in the U.S., sterilization remains all too available for women of color. The federal government stopped funding abortions in 1977, but it continues to pay for sterilizations. During the 1970s, women’s health activists exposed various forms of sterilization abuse (see section on sterilization in chapter 13, Birth Control). Since the 1980s, advocates have fought against new policies that coerce women with low incomes into using Norplant, a long-term hormonal contraceptive.
In the Third World, in addition to the widespread unavailability of desired contraceptives, there is a long history of coercive fertility control, primarily funded and inspired by developed countries, especially the U.S. (see chapter 26, The Global Politics of Women and Health, for the international dimensions of population control).
The right to abortion is part of every woman’s right to control her reproductive choices and her own life. We must reject all efforts to coerce women’s reproductive decisions. The goals of reproductive rights activists must encompass the right to have children as well as the right not to.
ABORTION ACCESS IN THE U.S.
- It is conservatively estimated that one in five Medicaid-eligible women who want an abortion cannot obtain one.
- In the U.S., 84% of all counties have no abortion services; of rural counties, 95% have no services.
- Nine in ten abortion providers are located in metropolitan areas.
- Only 17 states fund abortions.
- Only 12% of OB/GYN residency programs train in first-trimester abortions; only 7% in second-trimester abortions.
- Abortion is the most common OB/GYN surgical procedure; yet, almost half of graduating OB/GYN residents have never performed a first-trimester abortion.
- Thirty-nine states have parental involvement laws requiring minors to notify and/or obtain the consent of their parents in order to obtain an abortion.
- Twenty-one states require state-directed counseling before a woman may obtain an abortion. (This is often called “informed consent”; some critics call it a “biased information requirement.”)
- Many states require women seeking abortions to receive scripted lectures on fetal development, prenatal care, and adoption.
- Twelve states currently enforce mandatory waiting periods following state- directed counseling; this can result in long delays and higher costs.
- (Seven more states have delay laws which are enjoined–i.e., not enforced due to court action at the federal or state level.)
Note: for sources on these statistics, please consult the book’s notes at the end of this chapter.
ABORTION WORLDWIDE
Unsafe abortion is a major cause of death and health complications for women of child-bearing age. Whether or not an abortion is safe is determined in part by the legal status and restrictions, but also by medical practice, administrative requirements, the availability of trained practitioners, and facilities, funding, and public attitudes.
While it is difficult to get reliable data on illegal and unsafe abortion, several well-known organizations and researchers, including the World Health Organization, the Alan Guttmacher Institute, and Family Health International, make the following estimates:
- Worldwide, 20 million unsafe abortions are performed annually. This equals one unsafe abortion for every ten pregnancies and one unsafe abortion for every seven births.
- Ninety percent of unsafe abortions are in developing countries.
- One-third of all abortions worldwide are illegal. More than two-thirds of countries in the Southern Hemisphere have no access to safe, legal abortion.
- Estimates of the number of women who die worldwide from unsafe abortions each year range from 70,000 to 200,000. This means that between 13 and 20% of all maternal deaths are due to unsafe abortion–in some areas of the world, half of all maternal deaths. Of these deaths, 99% are in the developing world, and most are preventable.
- Half of all abortions take place outside the health care system.
- One-third of women seeking care for abortion complications are under the age of 20.
- About 40% of the world’s population has access to legal abortion (almost all in Europe, the former Soviet Union, and North America), although laws often require the consent of parents, state committees, or physicians.
- Worldwide, 21% of women may obtain legal abortions for social or economic reasons.
- Sixteen percent of women have access only when a woman’s health is at risk or in cases of rape, incest, or fetal defects.
- Five percent have access only in cases of rape, incest, or life endangerment.
- Eighteen percent have access only for life endangerment.
Did celebrity efforts like Band Aid’s “Do they know it’s Christmas?” and USA for Africa’s “We Are The World” actually help alleviate famine in the 1980s?

Some people will say that the musicians selflessly raised large amounts of money to help the world’s neediest. Others – myself included – would say that when projects like this don’t involve professional humanitarianism and the beneficiaries (i.e. the people who are supposedly being helped), the law of unintended consequences allows for the best of intentions to pave a road straight to H-E-double-hockeysticks.
There’s three broad ways that Celebrity Aid is often asserted as a success, or conversely, criticized as a failure. Namely they are (1) the amount of aid that actually hit the ground, (2) the stereotypes of Africans it created in the media, and (3) that they may have actually been complicity in ethnocide in the Sub-Saharan African context. I’ll address each separately.
(1) The amount of aid that hit the ground.
Band Aid famously started when Bob Geldof led the charge to raise money for famine in Ethiopia. Naturally, it was done with the best of intentions. The problem is that whereas most people think of famines as natural disasters they are in fact socio-political disasters. To put it another way, there are two models of famine, “food availability decline” and “food entitlement decline” (this is most famously discussed by Amartya Sen). In most cases of famine – for example Ethiopia in the 1980s – there was plenty of food available – the problem is that the poorest people didn’t have access to it, i.e. they weren’t “entitled” in the sense that they couldn’t afford it. When crops fail, there is usually still enough food around to feed people, however the reduced amount of food creates inflation, thus driving up prices. Dumping more money into a hurting economy doesn’t help this (see Dambisa Moyo or Paul Collier’s discussion of aid and Dutch Disease), it worsens things by putting more money in the hands of the wealthy. Additionally, don’t forget that a huge amount of the money raised goes to covering costs of holding these events (honorariums for the artists are a part of this). Much is further siphoned off on the way (including by governments, I’ll get to that in part 3). This is assuming that the aid that arrives is delivered professionally. Humanitarian actors have learned in the last two decades that projects not directly involving local beneficiaries are doomed to failure, and this is still rarely put into practice. Therefore, though millions of dollars are raised, much of it doesn’t hit the ground, and what does hit the ground is more likely to cause further damage and upset the local economy, than to actually save lives.
(2) Media portrayals of Africa
By showing lots of images of starving children with flies on their faces, the image of Africa becomes one of suffering and backwardness, rather than being a continent of diversity of life, culture, religion and experience that rivals that of any other. This video of a tract by Binyavanga Wainana (read by Amistad’s Djimoun Hounsou) describes this issue much better than I can. Basically, the image of Africa as the ‘dark continent’ full of savage warriors and starving babies is not an accurate depiction, and events like Band-Aid and We are the World perpetuate these not only false but outright racist depictions of life in the developing world. The interaction that most people have with “Africa” as a concept therefore becomes the starving child with the flies on its face, rather than learning of the history of the Mali Empire, the Songhai Great Zimbabwe, Shaka Zulu, or of learning the literature of Chinua Achebe or Wole Soyinka, or even learning the inspiration recent struggles of anyone from Nelson Mandela or Zackie Achmat amongst countless others. Instead, when you ask people what happens in Africa, you get the image of the starving child. Band Aid played a more central role than anything else in constructing this image.
(3) Complicity in mass murder and ethnocide
This is the most controversial aspect of Band Aid and related endeavours that there are. Many (including Tim Allen, Alex de Waal) have argued that Band Aid was directly complicit in the mass murder of hundreds of thousands of people. This is a highly contentious point. A brief history lesson: Ethiopia was ruled by the West’s darling Haile Sellasse, before he was ov3ertrhown by a nominally-Marxist ruler called Mengistu Haile Mariam. His party, known as the Derg, received support from the USSR. In the early 1980s, a group of Ethiopian ethnic minorities rose up against his rule (a larger one was the Oromo Liberation Front, although Eritrean groups were very active). When crops began to fail (this occurred cyclically, with the worst year being 1984), Mengistu blocked aid to the region, blocked refugees from leaving, as while limiting the international assistance that arrived. What assistance did arrive was taken by the regime, and not sent to the minority areas. Though the regime definitely didn’t cause the famine, they undoubtedly made it worse, using it as a cheap form of counterinsurgency (similar uses of famine as a form of counterinsurgency occurred in the Biafran War in Nigeria in the 1970s, and in Darfur in the 2000s). Support for “Ethiopia” became support for the Derg, and the famine it perpetuated in minority areas of Gojjam, Eritrea, Hararghe, Tigray, and Wollo. Basically, in their attempts to raise money for starving children, fundraising ended up providing legitimacy to the Ethiopian regime, while also sending it lots of money that was inevitably re-directed to other areas (especially corrupt politician’s pockets).Along with Operation Lifeline Sudan, and assistance in the Biafran War, the Live Aid / Band Aid exploits are held up as the three most famous examples of humanitarianism gone wrong, and the best of intentions being manipulated by local actors to pursue policies of ethnocide.
The idea that we must “do something” and that we must “save the world” is dangerous if you don’t deliver aid professionally, through professionalized humanitarian channels no embodied in organizations like MSF, Oxfam, etc., with the involvement of the beneficiaries on the ground. The rather embarrassing Band Aid saga speaks to this point as well as anything else. Good intentions and cash simply aren’t enough; we need to do better.
How much did Band Aid/ We are the World/Live aid help? The optimistic answer would be “not much”, while the cynical answer would be “it actually made things worse”. But the silver lining would be that it helped professional humanitarians (i.e. not musicians, but actual trained NGO staff) sharpen their game and improve their delivery, to avoid the disasters that come when you deliver aid in an unprofessional manner.
A Native American man inspects the newly completed transcontinental railroad, 1868.

There goes the neighborhood.
(Source)
If you’re every up for a REALLY depressing read on the history of the US — read Howard Zinn’s “A People’s History of the United States”
Parents march in support of their LGBT kids, New York City, 1974

Amazing how in 1974, when a celebrity or athlete coming out was unthinkable, to have parents in that day and age showing such support for their children. This picture illustrates not only common sense in loving a child who’s gay, but also immense courage in that time period.
Oppression Olympics

Example: comparing the suffering of Native Americans or European Jews. Each group had its own unique challenges and faced its own unique obstacles. Their persecution or repression evolved from vastly different trends and motivations in society. Short of the objective fact that being considered a piece of property and not a human being is one of the most dehumanizing and traumatic acts it is possible to impose on a person, it is better to look at, in my opinion, a broad struggle for equality within an impersonal legal framework supported by variously motivated establishment figures. Otherwise, you risk obscuring the suffering and struggles of one group because group X had it worse.
So, to conclude, certain acts may have been undeniably worse or more repressive, but to compare them to other groups is of dubious merit and risks starting a meaningless and historically irrelevant competition.
Why don’t people realize that we rise and fall as a unified society?

I think the main problem at large is that people have forgotten (or simply don’t realize) that by living as part of a society you inherently sign a social contract. Everyone born into any given social community is opted in automatically without choice or consent. What this means is that you are, by right, part of the community, you benefit from the community’s gains, and you are protected by that community. Now, you can opt out; only if you remove yourself from the social structure and stop taking the benefits provided (i.e. stop paying taxes, move to a different country with a different social structure, become a cave hermit in the remote wilderness) But if you don’t, then you have taken on a set of rules and a responsibility that coincide with the right to all due benefits (the chief responsibility of our society being the stupidly cliché and simplistic “golden rule.”) If every member of the community is eligible, then every member must be responsible to ensure the benefits’ continuous availability. (Although it partly is, this is not solely about money; also respect, security, safety, happiness, and human-rights etc…) This is where the misunderstanding comes in. You aren’t being an ‘evil-commie-socialist’ by giving back to society. It is required of you by the contract, but it’s also in your best interest.
The principle is not based on actual or perceived need, but on potential need. Obviously, there are people that need a lot, as well as people who need for nothing. The important point, though, is that everyone has roughly the same potential to end up in need. Anyone could get sick, anyone could get robbed or cheated, everyone needs access to get an education, everyone will die, anyone could be oppressed. That is the point of the contract; it’s why we have formed our society like this and not a cannibalistic anarchy. By ensuring none of these things could happen to the whole community you are ensuring they can’t ever happen to yourself. No matter how safe and sound you feel, no matter how impermeable or untouchable you think you are, no matter what your station in life may currently be; things change, and tragedy can strike anyone anywhere at anytime.
I’m not talking about a utopia, seriously, just a completely attainable place where people finally understand what it means to live in a community. Just play your part and pay in your share for the society that got you to where you are (You didn’t get there alone, be honest. Everything from your school, down to the road worker and garbage man are deserving of your respect and a return for their labor.) Just imagine, for a minute, a millionaire (whether his money comes from a company he built, his parents, the lottery, or back-breaking work,) he could only have accomplished it on the shoulders of the investors, engineers, teachers, gamblers, doctors or neighbors. That person would not be a millionaire if other people hadn’t held him up; If a doctor hadn’t delivered him or immunized him, if his neighbor didn’t respect or trust him, if a stranger hadn’t lost everything thereby making an opening or an opportunity, if there were no roads or trash collectors or farmers. With out the support of a society in people’s lives, it would be impossible for them to be “successful” in the way most people imagine it to be. There is too much work to be done and too much at stake to try and survive on your own. You can’t have an empire without resources, you can’t run a bank without customers, you can’t be a star without fans. When treating everyone else as less important than yourself, you convince them they aren’t needed and they will start to treat you the same.
Another thought, part of the problem with some of these people is that they haven’t really thought through their priorities. Some of them tie up their happiness in the pursuit of money. If you achieve gaining more money than you need, but you still need to gain more because that’s what makes you happy, isn’t the never ending cycle obvious? It will never be enough, so you will never be happy. Once you’ve gotten to the point that you’ve made so much money that you and each of your children could never spend all of in your lifetimes (and it’s still not “enough”) you should probably try and find something that would actually bring you meaning and happiness (how about instead of living for the profit, you live for the happiness your product brings, or the adventure of scientific discovery?) Wanting money and being rich aren’t inherently bad things, at all. But it is bad doing so for no other reason than selfishness. Not saying you should give all your money away (unless you want to…?) But don’t continue to make a sport of making money at the expense of your community without ensuring other people the same protection and support you had. To those who aren’t millionaires but still have plenty to be comfortable; I’m not saying you didn’t earn your comfort, but as I said before, it wasn’t only you that paid for it. Make sure you aren’t denying others the chance to have your level of health, happiness, comfort, or respect. Tomorrow your house could burn down, your bank could collapse, you could be diagnosed with a brain tumor, an earthquake could destroy your city, a silent majority could try and put you beneath them, or you could be ripped-off, raped or beaten. Where would you be then if society at large wasn’t a force to enable you to stand back up and fix the broken pieces.
A lot of these feelings of overestimated strength, egotistical independence, selfishness, and indifference, are products of an earlier era where these were needed. It was a time where only the strongest or most cunning genes would survive. But it is no longer beneficial to behave this way, we have vastly evolved from the small social groups requiring militant selfishness and ruthlessness. To behave like this now sets you apart from the “new” shift in social structure, which is based on strength in numbers. It damages your relationship with the community, leaving you vulnerable if you alienate yourself. Just because it was/is justifiable on the basis of animal instinct, doesn’t mean that we have to accept it. We have evolved a consciousness that is able to decide to not behave like animals. We can do the right thing for the sake of it being right, not just because it benefits us (which it ends up doing in this case anyway) In all honesty one person wont make or break it. Whether you decide to play along or not, you will still be enjoying all of the rights and privileges that the community tries to make sure everyone has. Until you’re not. If enough people decided to play the game on their own then society will fail. Not for some distant stranger, but for you. In that case, good luck. You’ll need it.
______________________________________________________________________________
I think Elizabeth Warren expressed my opinion on the social contract very well:
The Historians’ Case Against Gay Discrimination

Two historical propositions important to the legal analysis of discrimination of the LGBT community: (1) no consistent historical practice singles out same-sex behavior as “sodomy” subject to proscription, and (2) the governmental policy of classifying and discriminating against certain citizens on the basis of their homosexual status is an unprecedented project of the twentieth century, which is already being dismantled.
In colonial America, regulation of non-procreative sexual practices – regulation that carried harsh penalties but was rarely enforced – stemmed from Christian religious teachings and reflected the need for procreative sex to increase the population. Colonial sexual regulation included such non-procreative acts as masturbation, and sodomy laws applied equally to male-male, male-female, and human-animal sexual activity. “Sodomy” was not the equivalent of “homosexual conduct.” It was understood as a particular, discrete, act, not as an indication of a person’s sexuality or sexual orientation. Not until the end of the nineteenth century did lawmakers and medical writing recognize sexual “inversion” or what we would today call homosexuality. The phrase “homosexual sodomy” would have been literally incomprehensible to the Framers of the Constitution, for the very concept of homosexuality as a discrete psychological condition and source of personal identity was not available until the late 1800s. The Court in Bowers v. Hardwick misapprehended this history. Proscriptive laws designed to suppress all forms of nonprocreative and non-marital sexual conduct existed through much of the last millennium. Widespread discrimination against a class of people on the basis of their homosexual status developed only in the twentieth century, however, and peaked from the 1930s to the 1960s. Gay men and women were labeled “deviants,” “degenerates,” and “sex criminals” by the medical profession, government officials, and the mass media. The federal government banned the employment of homosexuals and insisted that its private contractors ferret out and dismiss their gay employees, many state governments prohibited gay people from being served in bars and restaurants, Hollywood prohibited the discussion of gay issues or the appearance of gay or lesbian characters in its films, and many municipalities launched police campaigns to suppress gay life. The authorities worked together to create or reinforce the belief that gay people were an inferior class to be shunned by other Americans. Sodomy laws that exclusively targeted same-sex couples were a development of the last third of the twentieth century and reflect this historically unprecedented concern to classify and penalize homosexuals as a subordinate class of citizens.
Since the 1960s, official and popular attitudes toward homosexuals have changed, though vestiges of old attitudes – such as the law at issue here – remain. Among other changes, the medical profession no longer stigmatizes homosexuality as a disease, prohibitions on employment of homosexuals have given way to antidiscrimination protections, gay characters have become common in movies and on television, 86 percent of Americans support gay rights legislation, and family law has come to recognize gays and lesbians as part of non-traditional families worthy of recognition. These changes have not gone uncontested, but a large majority of Americans have come to oppose discrimination against lesbians and gay men.
Obamacare vs. The World

Imagine the president of the United States saying they have a military target in their sights. If the US destroys this target it would save the country hundreds of billion dollars and tens of thousands of lives every single year. The target also appears to be vulnerable, there is little chance it could not be defeated. In fact, in recent decades other countries have defeated the same target with ease and great success. This mission would surely have the backing of the American people and be an immediate go. So what is the target? Is it North Korea? Iran? No, it is the private health insurance industry.
The US is the only rich country in the world without universal healthcare. This privatization of medicine causes the US to have the highest per capita medical costs and inferior outcomes. John Boehner stated in 2012 that America has “the best healthcare in the world.” Many Americans would agree with this statement but reality paints a much darker picture. The United States healthcare system was ranked 38th in 2000 by the World Health Organization. A 2012 report by the National Research Council and the Institute of Medicine ranked US dead last among 17 developed nations. Among these 1st world countries the US had the highest infant mortality rates, the shortest life expectancy, most injuries, most homicides and most disabilities. (So at least we’re #1 at something.) A Harvard study attributed 45,000 annual US deaths to a lack of health insurance. Families USA came to a more conservative estimate of 26,000 deaths from no insurance between the ages of 21-64. At the very least this is equivalent to suffering eight September 11th attacks, except these atrocities are self-inflicted and repeated every year. (3,000 Americans died from the 9/11 attacks so : 26,000/3,000= 8.67)
Let’s look at the economics of the issue. The US spent $8,233 per capita in 2010 according to OECD (Organization of Economic Cooperative Development) and $8,680 per capita on health annually in 2011. (Probably over $9,000 as of today – August 2013) For comparison Canada spent just under $4,500 per person in 2010. Our northern neighbors spend about half as much on healthcare and achieve superior results. The US spends 17.6% of it’s GDP on healthcare and the OECD average is 9.5%. This 8.1% differential in a 15 trillion dollar US economy amounts to over 1.2 trillion dollars. Routine operations frequently cost thousands of dollars more in the US than in other industrialized countries and we have the highest prices for pharmaceuticals. For example a coronary angioplasty average costs is $14,378 in the US and $5,547 is the average in Finland. Hip replacements are $5,000 cheaper on average in Canada and C-sections cost half as much in Germany. ($3,732 vs $7,449)
The health and lifestyle of Americans is similarly in terrible disrepair. The US has 5% of the world’s population and consumes two-thirds (67%) of the world’s anti-depressants. (Zolaft, Prozac) One in ten Americans are on these anti-depressant medications and the number of prescriptions is steadily climbing. The US also ranks at the top of the lists for anxiety disorders with over 40 million Americans being affected. Not surprisingly the lion’s share of the anxiety medication also get’s sold here. Our collective mental health is atrocious and our physical health isn’t much better. The US is always in the running for the world’s fattest country. Almost 70% of the US population is overweight and 30% of the population is obese. Heart disease, diabetes and high-blood pressure are frequent medical ailments costing hundreds of billions of dollars per year. The US has low rates of tobacco usage and yet still manages to have high cancer rates. As mentioned earlier, the US has the highest infant mortality rates, the shortest life expectancy, most injuries, most homicides and most disabilities among developed countries.
Implementing universal healthcare like every other industrialized nation is the obvious solution. It’s a political non-starter however. Bill Clinton chose to prioritize NAFTA over healthcare in 1993. He used up too much political capital getting the free trade bill passed and was unable to pass his healthcare bill. Fifteen years later Barack Obama was elected president and one of his first comments from the white house was that, “the public (healthcare) option is off the table.” Obama was able to get a health bill passed, The Affordable Care Act. The bill, dubbed Obamacare, does have some definite improvements. It will ensure greater coverage for Americans, end some of the insurance companies most exploitative practices and stem the tide of rampant medical inflation. Just as important though, the bill provides hundreds of billions of dollars in subsidies to health industries and leaves the root of the problem, privatized health insurance, intact.
Several studies have been conducted on implementing universal healthcare in America. Virtually all the studies have predicted colossal savings if the US were to adopt such a plan. Physicians for National Health Program have estimated annual savings at $400 billion dollars per year. In another estimate economist Gerald Freidman concluded single-payer healthcare would save $570 billion dollars annually. Among other nations Norway was the second biggest per capita spender in 2010 at $5,388, if the US could match this it would save almost 900 billion dollars per year. ($8,233-5,388= $2,845 per capita savings x 315,000,000 Americans = $896,175,000,000) This would be about 6% of US GDP. In actuality the US spends 17.6% of it’s GDP on healthcare which also the highest in the world. In second place is the Netherlands at 12.0%. If the US could just match this it would save 840 billion dollars per year. (17.6% – 12.0% = 5.6%) (5.6% x 15 trillion dollar US GDP = 840 billion dollars) The potential savings are enormous and are approaching a trillion dollars annually.
In addition to direct medical savings a single-payer system would eliminate the practice of medical bankruptcy. Medical bankruptcy is the number one cause of bankruptcy in the US despite the fact such a concept doesn’t even exist in other advanced countries. 60% of all US bankruptcies are from medical bills, affecting over 2 million Americans each year. Medical bills are attributed to 60% of all bankruptcies in the US and 25% of senior citizens will declare bankruptcy due to medical costs. Other benefits from universal care would be harder to quantify but just as real. Higher life expectancy, lower obesity rates, improved psychological health and improved infant mortality rates would all come along with lower costs. We’d also prevent tens of thousands of people from dying each year because they can’t afford treatment.
Let’s flip the script. Instead of trying to convince America to adopt universal healthcare imagine trying to convince a country with socialized medicine to Americanize their system. Really think about going to Japan and saying, “I understand that your country has a high life expectancy, low obesity rates and spends a little over $3,000 dollars per capita on healthcare. But as an American I see huge room for improvement. For starters you just can’t insure everybody, it makes people lazy and dependent. The poorest and unhealthiest 20,000 or so of your citizens should just be left out to die every year. There’s no profit to be made in treating them and hey we all gotta go sometime right? Even with them gone you’re still insuring too many people, it’d be best if you let about the bottom 1/6th of your population have little or no insurance at all – it’d be efficient and teach them personal responsibility. Also, your medical system has too little bureaucracy and is too easy to understand. Having everything under a single government payer is too streamlined with almost no overhead. You really want to break that up into several private insurance companies that deny as much coverage and claims as possible.” The Japanese would believe you are either joking or a complete psychopath, the system you are preaching for would seem like a sick joke.
For decades now a majority of Americans have wanted a single-payer system. Yet if a politician embraces single payer healthcare they are denounced as a left wing extremists. Obama was lambasted as a socialist for his modest reforms. In other countries this situation is reversed, only the extremists are opposed to single-payer healthcare. The health systems of western Europe are very popular with their citizens and rightfully so, they provide superior service at a lower cost. The US not only lags behind in cost and outcomes but also lags chronologically. South Korea had universal care in 1988. Denmark had it in 1973, Canada 1966 and Norway in 1912.
I can see a path from the Affordable Care Act to a universal single-payer health care system. Its psychological. As a nation, we are committed to making sure that every person receives health care affordably. If that’s the frame, then single payer starts making the most sense. The previous frame was that health care is an individual responsibility and if you didn’t have it then that was your problem. That’s a big difference. And I think that in politics, framing is key. How the population views an issue affects how they vote on it.
The Affordable Care Act is bad, but it’s so much better than what the previous system was. Children were dying because they hit their lifetime caps on insurance coverage before they were six. The Affordable Care Act fixed a lot of stuff but it didn’t go far enough. It’s not what the American people deserve but it’s what we could get.

***{( Their is a difference between the types of systems; here is some of them, along with the advantages/disadvantages and the challenges of adopting those types of systems in the US:
Single-payer insurance (Canada)
In this model healthcare remains provisioned by private parties but the government takes over the role of the insurer. This is the currently proposed alternative system in the US but the proposed version is very different to the Canadian model; In Canada doctors typically do not work for hospitals (they operate on a fee-for-service or time-fee basis as contractors to the Canadian government) and while hospitals are privately operated most of the buildings are provincially owned, neither of these are present in the proposed US model. This system can be free at point of use.
The health outcomes of this type of system are relatively good, although with some capacity issues which cause wait time issues. Short term such a switch would produce a saving of between 4% and 11% over the current system but the savings achieved would likely be reversed by an increase in consumption. This type of system also does nothing to address the wider problem of healthcare delivery.
While the contract based doctor provision is entirely achievable currently the way hospitals operate would not currently be possible, we don’t have the capital or borrowing capacity to purchase a sufficient number of hospitals off their owners and the constitution does not permit us to simply confiscate them without fair compensation.
Centralized Single-payer healthcare (UK)
In this model the central government controls facilities (although not always owns them, the UK has been experimenting with financing new facilities via PPP), personnel and financing with a central tax for healthcare provisioning. All doctors other then PCP’s typically work for the government (PCP’s are fee-for-service or time-fee). The UK is currently the only example of this in the developed world. This system is free at point of use.
Health outcomes of this type of system are average with significant capacity issues. There is no accurate prediction regarding the operating costs of this type of system in the US but it will certainly be smaller then current combined public & private spending and likely significantly so.
The problems with this type of system in the US would be numerous. Firstly centralized systems respond very poorly to regional changes in healthcare needs, this is one of the trade-offs for lower costs, and we would have to accept a lower standard of care (for those who do not currently have accessibility problems) then the current system overall in exchange for universal coverage and the lower costs (this is primarily why the UK system has not been repeated elsewhere). The problem with purchasing facilities is the same as with single-payer insurance.
Regional Single-payer healthcare (All the Nordic countries)
In this model the central government mandates the level of care regional authorities are required to offer and those regional authorities are responsible for raising the revenue and providing the services. As with centralized single-payer the facilities are generally owned by the government and doctors generally work for the government. This system is free at point of use.
Health outcomes of this type of system are good with few capacity issues. As with centralized single-payer it is not possible to accurately predict the operating costs of this type of system but they would also be lower then our current system while higher then centralized single-payer.
The only special problem with this type of system in the US is that its success lays in the relatively small size of its regional health authorities. The equivalent in the US would be the federal government mandating the service and a county taxing for the service and providing it, this would not currently be constitutional. Same facilities issue as the previous systems here.
Basic Single-payer healthcare (Australia)
Functions much the same as the Canadian example with the exceptions it is not always free at point of use (government pays between 75% and 100% of costs), the government does not cover most electives and there are a number of privately owned hospitals that treat public patients on a fee-for-service schedule.
Multi-payer (France, Germany etc)
Multi-payer systems differ from single-payer systems in numerous ways. Firstly healthcare is not supported from general tax revenues, the majority of healthcare is paid for via insurance or withholding specifically targeted at healthcare. Secondly the government generally neither owns nor operates the facilities, the overwhelming majority are privately owned and often operated for a profit (in the case of Germany nearly half the hospitals are operate for-profit compared to 12% in the US). Thirdly its not possible for the government to set a fixed healthcare spending level, single-payer systems establish how much they want to pay for healthcare and then distribute resources accordingly while multi-payer systems establish which services people are permitted to consume & the level of subsidy they will receive and spending is simply however much is consumed at those levels. This type of system is not generally free at point of use.
Health outcomes of this system vary but are generally very good and there are no capacity problems. It would be cheaper (how much depends on the exact form) then our current system while more expensive then the single-payer systems. There would be no particular problem replicating this type of system in the US but the tax and regulatory changes required could be challenging. This type of system would also be far more “free market” then the mess we currently have.
Third-party-payer (USA)
Absolute shit.
Account-payer (Singapore)
In account-payer systems patients pay for the majority of the healthcare out of pocket with a government subsidy applied (in effect if you are poor your heart transplant costs $50 while if you are wealthy it costs $50k), payments are made from savings accounts individuals are required to contribute to. This is not a free at point of use system.
Health outcomes of this type of system are very good and there are no capacity problems. Cost wise this would be the “best”, we would be able to fund a universal healthcare system while reducing current public healthcare spending. This type of system would also be far more “free market” then the mess we currently have.
(Universal and Single-payer are not interchangeable.)}***

So the USA pays approx DOUBLE the OECD average and yet manages not to have Universal Health Care. It’s a hell of an achievement. How can Americans pay for a Rolls Royce and yet take delivery of a Chevy with a puncture?
The USA needs to find the solution every other Western nation has found. Universal Health Care free at the point of delivery.
Why hasn’t it?
This is why. The Medical-Industrial Complex has donated $833,259,267 directly to members of Congress. Not counting the huge amounts of money given to presidential candidates like Obama, McCain and Kerry, the biggest donations have gone to the 3 worst industry shills who have been well-paid to make sure there will never be effective, robust health care reform:
Arlen Specter (R-D- PA- $4,026,933)
Max Baucus (DLC- MT- $2,833,731)
Mitch McConnell (R-KY- $2,758,468)
And when you just go right to Big Insurance, the non-presidential candidates who got the biggest legalized bribes were the 7 senators who have been tasked with the job of killing effective health care reform and keeping Healthcare Insurance alive in the USA
Ben Nelson (DLC-NE- $1,196,799)
Max Baucus (DLC- MT- $1,184,113)
Joe Lieberman (DLC- CT- $1,036,302)
Arlen Specter (R-D- PA- $1,035,530)
Mitch McConnell (R-KY- $929,207)
Chuck Grassley (R-IA- $884,724)
( This is a great resource for checking who’s funding your politician)

Citied Web Sources:
- Health Care In America
- The USA pays as much out of the public purse from taxes as the average OECD nation, more than nations like France, Germany, the UK, Sweden, yet unlike the average OECD nation does not have any form of universal coverage
- World health care Organization rankings by per capita spending
- World Health care Organization rankings by performance
